Share
The COVID-19 pandemic has brought into stark focus the need for data and the value of models to inform response strategies. Since March, the Centre has been working with the Johns Hopkins University Applied Physics Laboratory (APL) to develop a COVID-19 model adapted for use in humanitarian contexts.
- Access the code repository, including all the source code scripts necessary to run the model.
- View the technical documentation and FAQs explaining how to configure and run the source code in the repository.
- Download the methodology paper providing details on model assumptions and the main equations.
- Access biweekly reports for six countries.
- Download the OCHA-Bucky model card created according to the Centre’s Peer Review Framework.
The result is a model, named OCHA-Bucky, that forecasts the number of cases, hospitalizations, and deaths over two or four weeks, at the subnational and national levels. Below, we share the code and documentation for the model, releasing it as a public good so that our community can learn from our experience and extend the model for other uses and locations.
The guiding principle for developing the model has been to support short-term operational decision making in an effort to protect and save more lives in humanitarian crises. The model projections are available for six countries: Afghanistan, the Democratic Republic of Congo (DRC), Iraq, Somalia, South Sudan and Sudan. Since July, we have worked with OCHA colleagues and partners in these locations to finetune the model with country-specific data. We produce bi-weekly reports with projections and observations for each country.
Model Overview
As we have seen since the start of the COVID-19 pandemic, epidemic forecasting is one tool through which we can gain an understanding of the final outbreak size and an indication of when the epidemic may peak in a country. This provides decision-makers with the capability to plan and manage resources during a pandemic.
In March, OCHA and APL established a partnership to bring this type of foresight to humanitarian operations. We developed a series of adjustments to an existing COVID-19 model (JHUAPL-Bucky) that was developed as part of the Centers for Disease Control and Prevention (CDC) COVID-19 Mathematical Modeling Forecasting Ensemble. (The ‘Bucky’ part of the name comes from the name of the main developer’s cocker spaniel).
The resultant model, OCHA-Bucky, stratifies COVID-19 dynamics by age and population vulnerability. Input to the model consists of geographically distributed COVID-19 cases and deaths. Model output consists of future projections of these same quantities, as well as severe cases. The model considers both intra-regional mobility of the population and non-pharmaceutical interventions (NPIs).

The Main Takeaways
After months of developing the model and working with field-based colleagues to make it useful, we have five main takeaways, which are explained in more detail below.
1. Short-term projections, updated regularly, are more helpful
Given the dynamic nature of the disease, we knew that our model assumptions would need to evolve. At the beginning of the outbreak, COVID-19 was spreading in an uncontrolled way in many countries resulting in a high reproduction rate (a measure of how fast cases are growing). As governments implemented mitigation measures to slow the spread of the disease, the reproduction rate dropped.
In Somalia, for example, the initial estimated reproduction rate was about 3, and by late April this had changed to a much lower value (see visual below). Given this dynamic situation, projections made in February and March were no longer applicable to the observed situation in April and onwards.

For this reason and based on requests from OCHA country offices, we decided to focus on short-term projections that could be used to inform immediate operations. In OCHA-Bucky, the reproduction rate is estimated from the latest cases and deaths data reported by WHO and Ministries of Public Health.
2. The projections need to account for reporting challenges and risk-factors specific to humanitarian crises
By now, we have become familiar with the COVID-19 data reported by the authorities and we are more aware of the gaps and reporting delays. OCHA-Bucky uses recent data to estimate the fraction of cases expected to be reported and corrects the projections to account for large underreporting observed in these countries.
Drawing from existing evidence in scientific literature and specific to humanitarian contexts, we include food insecurity and indoor air pollution as risk factors in the model. For example, there is evidence that weight impacts the severity of influenza and other respiratory viruses. Hence, we scale our vulnerability factor by levels of food security within a region. (Food insecurity data is obtained from the Integrated Food Security Phase Classification). The proportion of individuals living in regions at IPC level 3 or greater are considered at-risk.
3. Subnational projections are critical to inform operational decisions
The first COVID-19 projections produced globally had one projected number for cases and deaths for the entire country with no sub-national breakdown (see the work done by the London School of Hygiene and Tropical Medicine and Imperial College of London). These national projections are helpful for getting an understanding of the overall scale of the crisis but have limited use for targeting interventions within a country.
There have been two challenges in producing subnational projections: data availability and technical model limitations. The HDX team manually extracts subnational data from government sources, a time-consuming process. For the model, we designed OCHA-Bucky to estimate the main parameters at the subnational level from the latest reported data.
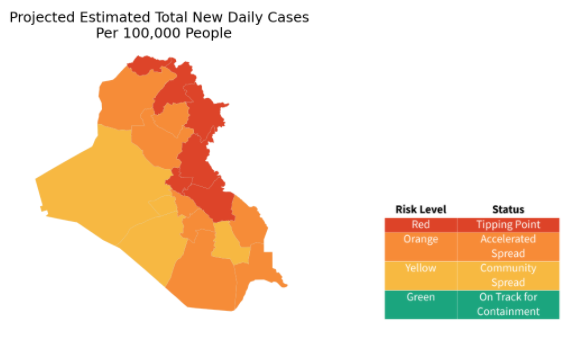
Having subnational projections for Iraq, for instance, allowed us to identify a spike in overall cases that was mostly due to large increases in Baghdad and a few other governorates in the northeast of the country. In addition, the subnational trends showed that despite a decrease in the number of daily new cases, suggesting an improvement, some governorates were still in a concerning situation.
4. Decision-makers need a simulation tool
In the six countries that we are focused on, measures to mitigate the spread of the virus are being applied at the city or county level, with very few measures applied nationally. Because of this, we designed OCHA-Bucky in a way that accounts for the type of NPIs in place in different regions, along with an estimated compliance level for each measure. Decision-makers can use the model to explore the effect of certain measures on the projected number of cases, hospitalizations and deaths.
5. Results should be presented in a practical manner
Communicating the results of the model is as important as the results themselves. Our biweekly reports include key messages about the latest model projections as well as the limitations with the data. The reports include both national and subnational metrics and we translate the projections into risk levels in order to support response strategies. This is based on the guidance developed by the Harvard Global Health Institute, Harvard’s Edmond J. Safra Center for Ethics and their partners.
Next steps
We are submitting OCHA-Bucky for an independent technical and ethical peer review based on the Centre’s Peer Review Framework. In parallel, we will continue to run the model every two weeks for as long as it’s useful. In line with the priorities identified by OCHA country offices, we are also looking at potential extensions of our analysis to understand the secondary impacts of COVID-19 on vulnerable populations.
We would like to thank OCHA colleagues in Afghanistan, Iraq, DRC, Somalia, South Sudan and Sudan for their engagement throughout this process. We also recognize the value of having a strong technical partner like APL and thank them for their extraordinary support.
This work would not be possible without financial contributions from a number of partners. We would especially like to thank The Rockefeller Foundation for its early investment in the OCHA-Bucky model which allowed us to accelerate our efforts at a critical time. We are also grateful to the Governments of the Netherlands, Germany, Belgium and the United Kingdom, as well as the municipality of The Hague, for their support to the Centre’s predictive analytics workstream and the work of the Centre more broadly.
If you have any questions or feedback, contact us at centrehumdata@un.org.